

Trade Idea - Short Pfizer (PFE)
"Safe & Effective" Or "Sentinel Event"...?

**NOT FINANCIAL ADVICE. This is a trade idea created to provoke thought and discussion**
Intro:
I’ve put this piece together as a thought process, and to help others evaluate an underpriced opportunity that may be presenting itself to those with eagle eyes and a nose for profit. Several hours will be needed to consume this blog and the links contained within, particularly ‘The Science’ section. You may wish to break this down into several visits to evaluate each section before proceeding to the next. Alternatively you can skip to the ‘Trade Idea Summary’ and ‘The Trade’ sections at the end.
The central thesis is that the Pfizer COVID-19 mRNA vaccines may be causing more harm than good, and that the general public, national health bodies and governments may be sleeping at the wheel of a global public health crisis. I understand that this is a controversial opinion, and that there are sensitivities at play here, given the official narrative of the COVID-19 vaccines being the saviour of society, and the one way ticket out of the pandemic.
Below I will present a combination of medical/scientific evidence/opinion, clinical research data, analysis of excess death data particularly in the US and UK, and evidence of clinical trial malpractice/fraud. I will provide links to the work/research of others, cite them and recommend you follow them to monitor the progress of this idea over the coming 12 months.
There are several contributing factors at play to this idea, which combined create a compelling case for the short. These contributing factors are broken down below into different themes for consideration. I have not done the heavy lifting here, only pulled together the work of others into a single blog to streamline a case for the trade.
Why mRNA Vaccines Are Different:
The first key point to understand is that mRNA vaccines are not the same as traditional vaccines. Traditional vaccines typically use a ‘Live Attenuated Virus’ technology, basically injecting a weakened or dead virus into the body of a defined dosage, to allow the body to create an immune response to the static dose, and develop antibodies.
has created an incredibly detailed and descriptive Substack blog which articulates the differences between traditional and mRNA vaccine technologies. ARK Medic can also be found on Twitter under the monicker @Jikkyleaks. I would strongly recommend giving them a follow, given the depth of knowledge and attention to detail in their investigative work. I must state that although I go by the monicker ‘ARK’, I am not ARKMedic, nor have I ever met them. :-) Anyway, here’s the link to the Substack blog below…There are 18 key differences articulated in the incredibly detailed and diligent blog above. However the key takeaways for the layman are points 1, 4, 12 and 18. There is no way to definitively regulate the amount of spike protein that is produced by the protein synthesis once mRNA translation occurs. Nor to definitively regulate how long the vaccine spike protein mRNA and vaccine spike protein itself remain in the body post inoculation. Nor is there any way to be 100% certain that the COVID-19 spike protein is synthesised from the mRNA in all recipients. There will be more on these above points discussed in the ‘The Science’ section below.
Trial Malpractice/Data (Brook Jackson):
When evaluating the diligence/integrity of the COVID-19 vaccine clinical trials, it is important to understand the health authority/regulatory recommendations/guidance for clinical trials, against which the COVID-19 vaccine clinical trials can be compared. The Food & Drug Admimistration of the United States recommends that a cautious, diligent clinical trial should take place over approximately five years before making a medication/product available to the general public.

Given the global desire for an expedient solution to the COVID-19 pandemic, the clinical trial process for the COVID-19 vaccines lasted less than 12 months before population wide rollout commenced in early 2021. In the midst of the expedited clinical trials, Brook Jackson came forward in November 2021 as a whistleblower highlighting the malpractice and potential fraud observed in the clinical trial process by subcontractor Ventavia Research Group. A detailed breakdown of her findings can be found at the British Medical Journal publication below.
https://www.bmj.com/content/375/bmj.n2635
Brook currently has a court case filed against Ventavia and Pfizer in the United States, which is currently ongoing. The outcome of this case could set the wheels in motion of a class action lawsuit against them, which I cover later in the ‘Idea Summary’ section.
https://www.bmj.com/content/375/bmj.n2635#media-1
Public Health Failings In Data Collection & Guidance:
Coupled with the potential clinical trial issues, was the failing of public health authorities to disclose full COVID-19 datasets. The Center For Disease Control & Prevention (CDC) in the United States was found to have withheld swathes of COVID-19 data. This means that any clinical / academic COVID-19/vaccine related research/evaluation using CDC data is compromised, and skewed bias potentially introduced into the published papers by these incomplete datasets. This could have resulted in the efficacy/safety of the COVID-19 vaccines being exaggerated. Since the below article is behind a paywall, you can use archive.ph, and paste the URL link in to access the article.

One of the key public health messages to instill mRNA vaccine safety confidence, was that the COVID-19 vaccine spike mNRA would be broken down by the body and removed ‘within a few days’. Last August, DiscloseTV discovered that the CDC had removed the guidance from their website without public disclosure. There has been no public explanation from the CDC to this day, as to why this guidance was removed from their website.

The Science:
How Long Does The vaccine spike mRNA Remain In The Body?
One of the reasons for the CDC removing the above guidance from their website, may be the paper by Roltgen, Nielsen et al published in January of last year. They found that the vaccine spike mRNA and vaccine spike protein were detected in the Lymph node germinal centres 55-60 days post vaccination in vivo. This was not known at the time of the clinical trials, or if it was, this information was not included in the vaccine Emergency Use Authorisation (EUA) submissions. This indicates that the regulation over how long the vaccine mRNA & spike protein remain in the body is unknown. The spike mRNA could be produced in the body over a prolonged period, potentially creating inflammation, elevated immune responses & chronic immunity issues in the individual.

What Happens When You Use N1-MethylPseudoUridine In The Vaccine mRNA?
The COVID-19 mRNA vaccines replace the natural amino acid Uridine with the synthetic N1-MethylPseudoUridine in its spike protein mRNA amino acid sequence. This is an intentional insert, because N1-MethylPseudoUridine helps to stabilise the otherwise fragile and easily degraded mRNA. There are however two important implications to using N1-MethylPseudoUridine in mRNA sequences that can create the risk of elongated and/or misfolded proteins:
Amino Acid mutations creating a different amino acid sequence, and potentially a different protein synthesised than the spike protein. This protein could be benign. It could be more harmful. There is no way to determine what is produced in these instances due to the random nature of amino acid mutations. The most eye catching part from the Nature paper by Chen, Potapov et al linked above can be found below:

Stop codon readthroughs. Stop codons are a group of 3 amino acids that control when a ribosome should stop translating the mRNA, terminating the protein synthesis process. Using N1-MethylPsuedoUridine in the amino acid sequence can risk stop codon readthrough, causing mRNA translation and protein synthesis to continue beyond the stop codon, creating a different protein than the one intended. It is unknown what level of analysis into the use of N1-MethylPseudoUridine & stop codon readthroughs was undertaken during the clinical trials.

What Is The Biodistribution Of The Lipid Nanoparticles Post Injection?
The COVID-19 mRNA vaccines are transported in the body in a Lipid Nanoparticle (LNP) envelope. These are neutrally charged fatty envelopes that enable the mRNA to be transfected into cells for mRNA translation and spike protein synthesis to occur. In theory, once the LNP envelopes transfect the cell, they become ionised, which causes breakdown of the LNP & release of the mRNA.
The Substack/Twitter user
has created and incredibly detailed analysis of the LNP technology, what we know, what we don't know & potential limitations. While much of it may go over the Layman’s head, I’ve linked a couple of key images below from the blog, and you may wish to skip to the end section: “How mature is LNP technology” for the summary.

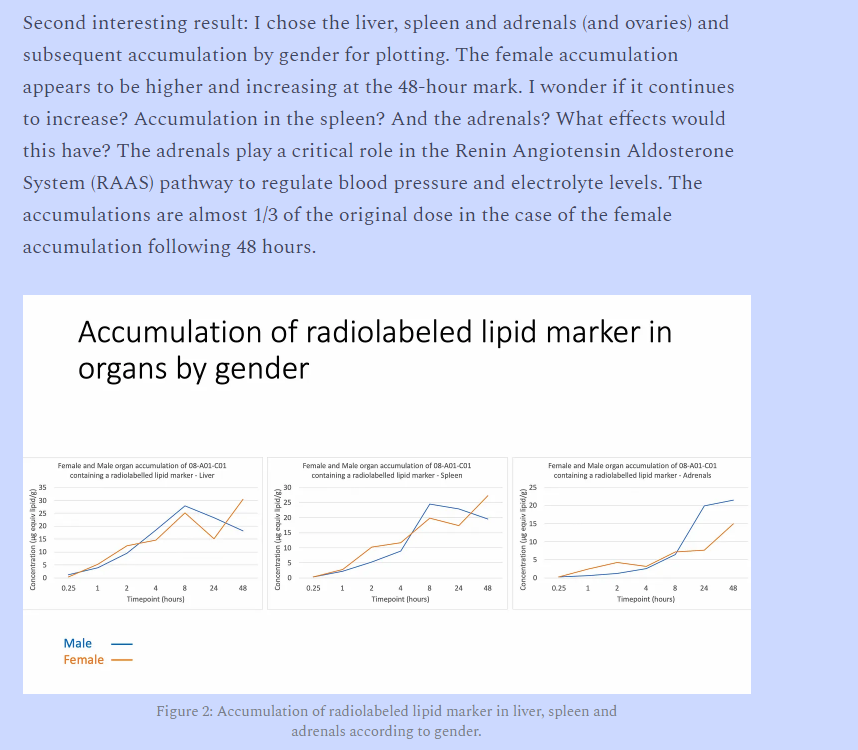
Coupled to this thesis, Jessica Rose (Twitter: @JesslovesMJK) has undertaken extensive work reviewing the Pfizer clinical trial data, particularly the trials on mice and the biodistribution found within. The result of these trial findings, is to confirm that the vaccine mRNA/spike protein does not remain at the injection site, and is located in multiple organs throughout the body only hours after inoculation. This indicates that there is little to no regulation/control of where in the body the vaccine spike mRNA/spike protein can end up.
Do More Boosters Equal More Infection?
Cleveland Clinic recently released a preprint study of their ~51,000 employees that indicates the more one vaccinates against COVID-19, the more likely they are to contract infection. While this is a preprint pending peer review, Cleveland Clinic is one of the most highly regarded health systems in the world, and their findings should not be taken lightly.

The above findings in the US are also supported by the New South Wales data coming from Australia, thanks to Twitter user @LCHF_Matt for their extensive analysis and for sharing the thread.

Does Repeat Injection Cause Autoimmunity?
Two separate papers have recently been published from different countries by Irrgana el al here and Buhre et al here, disclosing a transition from IG3 to IG4 antibody expression when an individual undertakes repeat COVID-19 doses. This can cause the immune system to ignore rather than attack the spike protein, prolonging and proliferating its existence in the body, and potentially causing organ inflammation that could cause chronic conditions or death in extreme cases. Twitter user
does a great job of kindly breaking this down for the layman here.
Myocarditis Links:
Myocarditis is a well documented link with the COVID-19 mRNA vaccines, and debate remains over whether it is the virus, the vaccines or both that are contributing to these diagnoses. There are, in the author’s opinion, several signals amongst the noise that indicate that the mRNA vaccines may be the dominant cause of the increases in cardiac/Myocaridits cases since the pandemic began.
The Australian Department of Health (DOH) introduced through its Medicare Benefits Schedule (MBS), an MRI test dedicated to detecting mRNA vaccine induced Myocarditis in borderline outlier cases. This test was assigned service code 63399 and was commissioned from 1st January 2022, to last 12 months.
This service code 63399, as of December 2022, has been claimed for over 1500 times between January and November, before the December data is added to the database.

Last month, the DOH decided to continue the availability of the test until December 2023, indicating that this is a trend they anticipate the continue.

It’s important to consider that this test is used in outlier, borderline instances when traditional methods to detect mRNA vaccine induced Myocarditis fail. The actual number of confirmed cases of mRNA vaccine induced Myocarditis could be much higher. It is also important to consider that there is no service code commissioned for COVID-19 infection induced Myocarditis, indicating that the Australian DOH has an inclination as to what is definitively causing the increase in cases of Myocarditis…



This study from Israel by Tuavli et al on almost 200,000 patients determined that COVID-19 infection/recovery had no effect on the instance of Myocarditis/Pericarditis.

This study from the Nordic region by Karlstad et al on a sample size of 23.1 million residents, showed an elevated risk of Myocarditis in young males, particularly after the second dose of the mRNA vaccine.


Global Excess Deaths:
It is no secret that excess deaths globally have been elevated following the COVID-19 pandemic. The puzzling question is, why 3 years into the pandemic, as the virus has become more benign and is causing fewer fatalities, are excess deaths not due to COVID-19 infection still elevated?
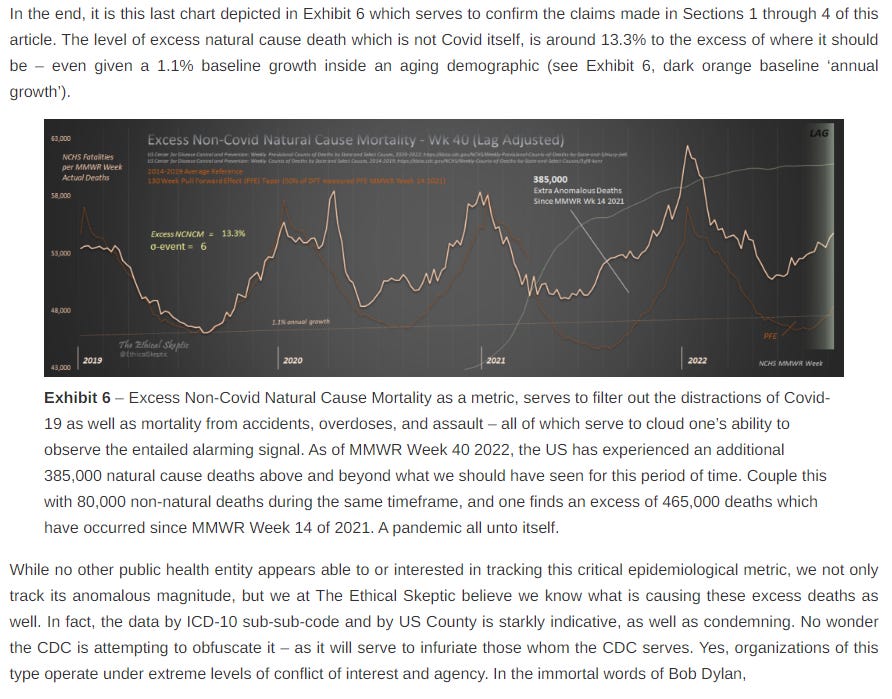
@EthicalSkeptic can be followed on Twitter, and has performed extensive analysis of the CDC’s ‘All Cause Mortality’ data, categorising deaths by ICD10 code, updating their analysis frequently as new data is released. While the CDC data should be taken with a pinch of salt per the ‘Public Health Failings’ section above, the two below blog posts are integral reading to understand their statistical analysis and findings. According to @EthicalSkeptic, something changed around April 2021, which has caused the excess deaths to remain elevated from the baseline trend ever since. These blogs are long, detailed reads, but I have screenshotted the key findings from both below for brevity.

Houston, The CDC Has A Problem
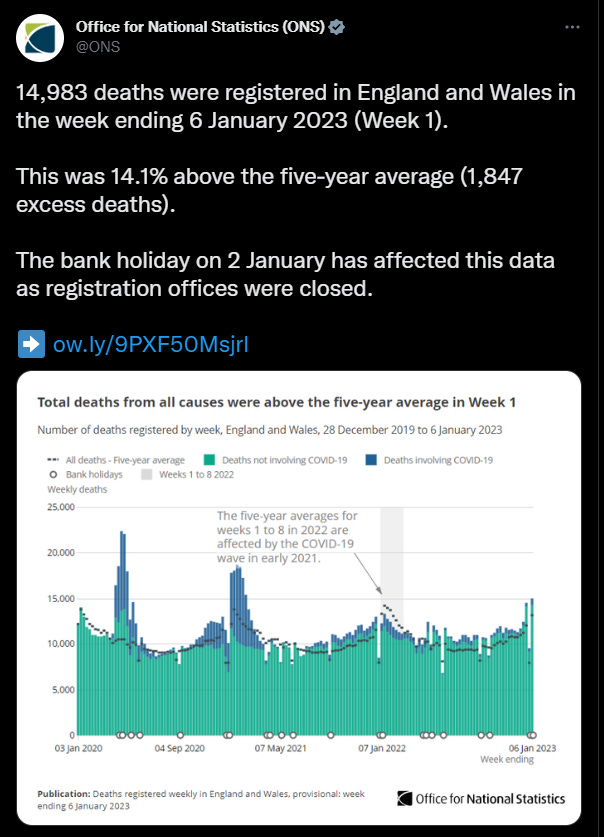
The UK’s Office For National Statistics themselves acknowledge the excess deaths in the first week of January 2023, with a 14.3% elevation above the baseline trend, and almost 15,000 during the week.
The EuroMOMO excess deaths data, which tracks excess deaths across 25 countries in Europe, also remains elevated above baseline. It is important to note that the scale of this elevation is being artificially suppressed by EuroMOMO, by not including COVID-19 pandemic years in their baseline trend.

More Doctors Speaking Out:
More and more doctors continue to speak out raising their concerns with the COVID-19 mRNA vaccines. Several videos are linked below from prominent doctors for the reader’s consumption.
Dr. Keryn Phelps is the former President of the Australian Medical Association, and her standing in Australian health & politics is unrivalled. It is telling that she has spoken out in this way. It is particularly important to pay attention to her warning that doctors are afraid to speak out under threat from the public health authorities such as AHPRA. This indicates that the problems caused by the mRNA vaccines might be worse than currently understood/communicated because doctors cannot speak freely on the subject.
Dr. Aseem Malhotra is a Consultant Cardiologist was originally a COVID-19 mRNA vaccine supporter, who changed their position on the safety and efficacy of the COVID-19 mRNA vaccines after scrutinising the Pfizer clinical trial data.
Dr. Peter McCullough is one of the most published Cardiologists in medical history, and has long been a critic of the COVID-19 mRNA vaccines.
Dr. Paul Offit, a member of the FDA vaccine advisory board is now voting against Bivalent boosters based on the lack of efficacy.
Dr. Joseph Ladapo, Florida Surgeon General, changed guidance for COVID-19 mRNA vaccinations late last year, particularly in men aged 18-39.
The above doctors are tenured, published medics, several of whom serve in leading positions with regional/national health authorities/regulatory bodies. Their medical opinions should be taken seriously.
Trade Idea Summary:
It is not any single theme from the above, but rather all the themes combined collectively that make this a compelling trade idea.
In summary, due to:
No control/regulation over how long the vaccine spike mRNA remains in the body.
No control/regulation over how long the vaccine spike protein remains in the body once synthesised.
No control/regulation over the concentration of vaccine spike protein synthesised from the vaccine mRNA.
No control/regulation over vaccine spike mRNA amino acid mutations that could cause protein elongation/misfolding.
No control/regulation of the Lipid Nanoparticle biodistributon in the body.
No control/regulation of the Lipid Nanoparticle toxicity in the body.
The risk of autoimmunity created by repeat inoculation of COVID-19 mRNA vaccines & implications for chronic disease contraction.
The Australian DOH’s service code 63399 being claimed for over 1500 times in 2022.
The possibility that COVID-19 mRNA vaccine safety & efficacy has been exaggerated by clinical trial research created from incomplete datasets causing skewed bias.
The possibility that malpractice and fraud occurred during the Pfizer mRNA vaccine clinical trials.
The continued elevation of excess deaths from baseline trend globally over 3 years into the COVID-19 pandemic, despite the virus mutations to a more benign variant and fewer COVID-19 deaths.
More and more prominent doctors speaking out about the prevalence of mRNA vaccine injuries, including the former President of the Australian Medical Association, who highlighted that doctors are afraid to speak on over fear of regulatory body reprisal.
It is the author’s contention that rather than COVID-19 infection/”Long COVID”, it is in fact the mRNA vaccines that are the dominant cause of the elevated excess deaths and chronic injuries suffered by the population in the wake of the COVID-19 pandemic. The alpha in this trade is that the general public, national health authorities and governments are still not accepting of this reality,
It is also the author’s contention that throughout the course of 2023:
As excess deaths continue to remain elevated from baseline trend as COVID-19 deaths decrease/flatline.
As more doctors/scientists speak out against the risks of the COVID-19 mRNA vaccines.
As more whistleblowers come forward to expose clinical trial fraud/malpractice.
The outcome of Brook Jackson’s lawsuit against Pfizer/Ventavia becomes known.
Pfizer will lose their legal indemnity as a result of the revealed malpractice/negligence, and an incensed general public will demand their governments bring class action lawsuits against Pfizer. These lawsuits will stretch into the hundreds of billions of dollars, given the number of countries that procured the Pfizer mRNA vaccines, and the number of doses administered globally. Pfizer paid $2.3 billion in 2009 to settle a medical fraud case.
What would the cost of the biggest medical fraud in history, committed on a global scale be…?
The Trade:
Ticker: PFE (NYSE)
Current Share Price: $44.96
Market Cap: $252.37bn
Q3 Revenue: $22.64bn
Q3 Net Profit: $8.61bn
Q3 Net Change In Cash: -$487m
Q3 Cash On Hand: UNAVAILABLE
Option: PUT
Put Qty: 100
Strike Price: $22.50
Expiry Date: 19th Jan 2024
Position Cost: ~$2,000
Target Price: What price target can one put on potentially the largest medical fraud in history conducted on a global scale? :~) A sharp 70-80% drop in price from current price would provide a price target of $9-13 per share.
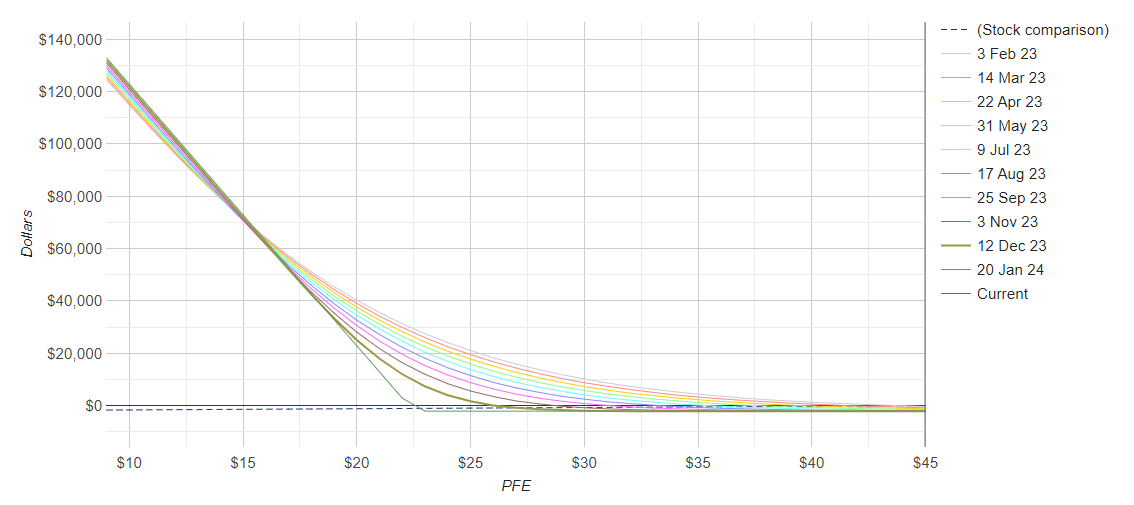
Position Reasoning: It is the author’s reasoning, that this idea will play out over a number of months, perhaps the full calendar year as the reality of the mRNA vaccine harms becomes prevalent. Therefore, a long expiration is desired to reduce the impact of theta decay on the position. 19th January 2024 is ideal, and the $22.5 strike price is currently cheap enough to enable a relatively large position to be undertaken for a relatively small capital allocation. This also allows for a scenario where if a conservative drop in price of ~50% occurs, the position shall still be in the money. The above reasoning could also receive tailwinds from current macro economic conditions, where elevated interest rates against current debt levels could cause a credit/liquidity event.
Effect of return on position is reflected in the graphic below.
To get a move of this size would need a court to rule that Pfizer committed fraud It will take years before this gets close to that point. Would love to be wrong
Excellent article.